Aesthetic chills mitigate maladaptive cognition in depression
Get The Article Article PDF BMC Psychiatry Article Aesthetic Chills Mitigate Maladaptive Cognition in Depression Cite This Work APA MLA Bibtex Schoeller, F., Jain, A., Adrien, V., Maes, P., & Reggente, N. (2024). Aesthetic chills mitigate maladaptive cognition in depression. BMC Psychiatry, 24(1). https://doi.org/10.1186/s12888-023-05476-3 “Aesthetic Chills Mitigate Maladaptive Cognition in Depression.” BMC Psychiatry, vol. 24, no. 1, Jan. […]
Current State of Potential Mechanisms Supporting Low-Intensity Focused Ultrasound for Neuromodulation
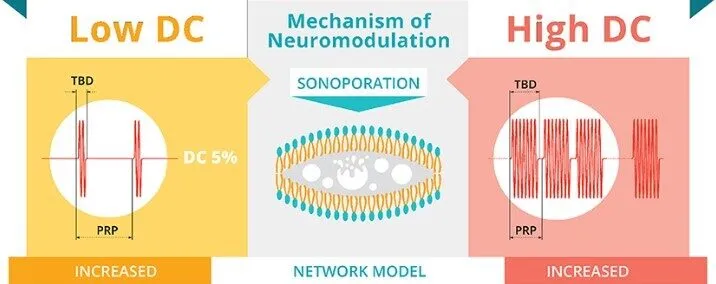
Published in Frontiers in Human Neuroscience in 2022, this review intended to answer how ultrasound for neuromodulation works Our review titled, Current state of potential mechanisms supporting low intensity focused ultrasound for neuromodulation, attempts to address the following questions: 1) How can we alter the amount of mechanical energy or other properties of the mechanical energy using the sonication […]
Frontiers Research Collection: Possible Applications of Neuroaesthetics To Normal and Pathological Behaviour
Dr. Felix Schoeller is now a Topic Editor for the Frontiers Research Collection under the topic: Possible Applications of Neuroaesthetics To Normal and Pathological Behaviour See The Research Collection Research Collection Possible Applications of Neuroaesthetics To Normal and Pathological Behaviour Research Collection Frontiers Research Collection: Possible Applications of Neuroaesthetics To Normal and Pathological Behaviour The […]
Cognitive Science Below the Neck: Toward an Integrative Account of Consciousness in the Body

Get The Article PDF Paywalled Article Cognitive Science Below the Neck: Toward an Integrative Account of Consciousness in the Body PDF Cognitive Science Below the Neck: Toward an Integrative Account of Consciousness in the Body Article Cite This Work APA MLA Chicago Harvard Vancouver Christov‐Moore, L., Jinich‐Diamant, A., Safron, A., Lynch, C., & Reggente, N. […]
New research sheds fresh light on mystery of infant consciousness

Get The Article Article PDF Trends in Cognitive Science Article Consciousness in the cradle: on the emergence of infant experience Cite This Work APA MLA Bibtex Bayne, T., Frohlich, J., Cusack, R., Moser, J., & Naci, L. (2023). Consciousness in the cradle: on the emergence of infant experience. Trends in Cognitive Sciences. Bayne, Tim, et al. […]
Interoceptive Technologies for Psychiatric Interventions: A Comprehensive Review
Get The Article Article PDF ScienceDirect Article Interoceptive Technologies for Psychiatric Interventions: A Comprehensive Review Cite This Work APA MLA Bibtex Schoeller, F., Horowitz, A. H., Jain, A., Maes, P., Reggente, N., Christov-Moore, L., . . . Friston, K. J. (2024). Interoceptive technologies for psychiatric interventions: From diagnosis to clinical applications. Neuroscience & Biobehavioral Reviews, 156, 105478. […]